Whether you’re a pitcher, swimmer, or tennis player or simply someone who reaches for coffee mugs and puts on shirts, the sharp pinch of shoulder pain when you lift your arm overhead can stop your life in its tracks. For athletes, that pain threatens your sport. For everyone else, it threatens your independence. And if you’ve been told “it’s just rotator cuff tendinopathy,” you might be getting an incomplete answer.
At Redbird Wellness in Hopkins, we see rotator cuff tendinopathy differently. We use scraping (IASTM), a precise, evidence-informed manual therapy, to address the tendon directly, stimulate its repair, and get you back to pain-free overhead motion without relying solely on heavy weights or surgery. But first, let’s clear up some confusion.
Part 1: What Rotator Cuff Tendinopathy Actually Is (And Isn’t)
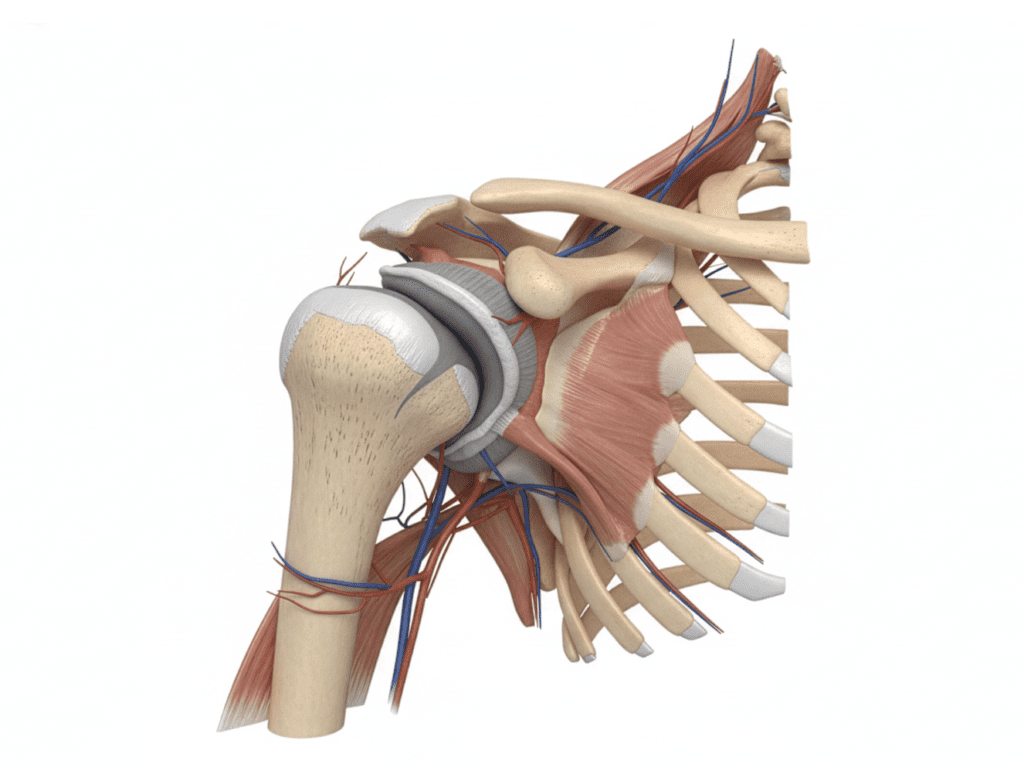
“Rotator cuff tendinopathy” gets thrown around loosely. Not all shoulder pain is rotator cuff tendinopathy. The term should be reserved for a specific problem: supraspinatus tendinopathy (the supraspinatus is the most commonly affected tendon, responsible for initiating arm abduction and stabilizing the humeral head during overhead motion).
Here’s why the distinction matters:
- Many older adults develop chronic impingement over years; scapular dyskinesis, thoracic stiffness, and altered mechanics gradually degrade the tendon. Their tendinopathy is the end result of a mechanical environment problem.
- Younger athletes (throwers, swimmers, tennis players) often develop tendinopathy from dynamic overload; repetitive high-speed eccentric loading during the deceleration phase of a throw, or the repetitive arc of a swim stroke.
Both are real. Both are painful. But their causes, and therefore their treatments, differ. A proper assessment (which we always perform) is essential before any treatment begins.
What this post is NOT for: If you have been told you have a full-thickness rotator cuff tear, this approach is not for you. Full-thickness tears in active individuals often require surgical consultation. Scraping is not a substitute for surgery in these cases.
What often gets missed is that rotator cuff tendinopathy rarely exists in isolation. The shoulder does not function on its own. It relies heavily on the coordination of the thoracic spine, rib cage, scapula, and even the core. If those systems are not contributing properly, the rotator cuff ends up doing more than its job, absorbing force it was never meant to handle repeatedly. Over time, that overload shows up as irritation, pain, and decreased tolerance to movement.
This is why people often feel confused when rest doesn’t fully solve the issue. You can reduce irritation temporarily, but if the underlying movement pattern doesn’t change, the same stress returns the moment you go back to normal activity.
Part 2: How Scraping (IASTM) Works
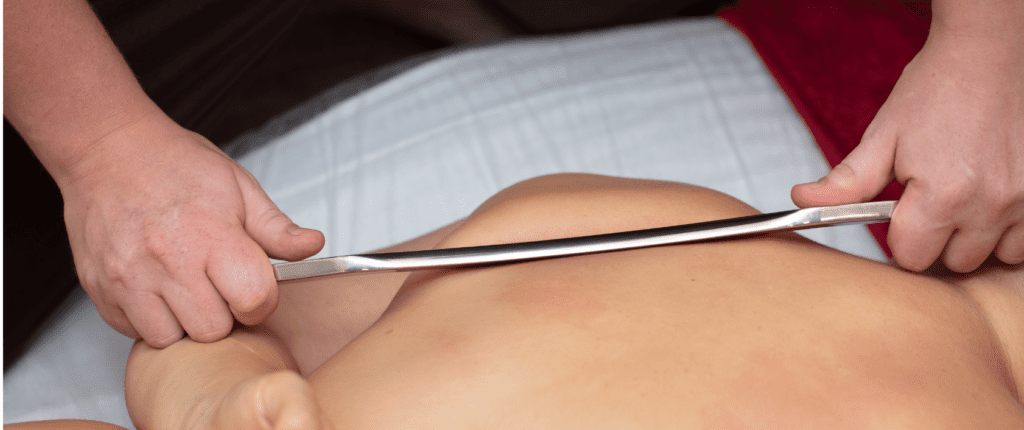
Scraping is a form of Instrument-Assisted Soft Tissue Mobilization (IASTM), the broad category that also includes cupping and dry needling. Within that category, scraping specifically uses a smooth-edged, stainless steel tool to apply compressive mechanical tension to the tissues.
Here’s what that pressure does:
- Cellular Changes
The controlled microtrauma from scraping triggers mechanotransduction, the process by which your cells convert mechanical forces into biochemical signals. Tenocytes (tendon cells) respond by increasing protein synthesis and collagen production. In simpler terms: the scrape “wakes up” the tendon’s repair mechanisms. - Tissue Changes
The compressive load helps remodel disorganized collagen, breaking up cross-links and adhesions that form in chronically irritated tendons. This restores the tendon’s ability to glide and tolerate load. - Neurological Changes
The mechanical input activates sensory receptors in the skin and fascia, which can “gate” pain signals at the spinal cord level. This reduces the sensitivity of the nervous system to the tendon, making movement less painful.
The key takeaway: Scraping provides an external mechanical load to the tendon at a level the patient can tolerate often when they cannot yet load the tendon sufficiently with weights alone. It’s not a replacement for strength training; it’s an adjunct that allows you to build capacity from a lower starting point.
Though that is important, another important piece here is dosage. Tendons respond best to progressive, controlled loading, not complete rest and not aggressive overload. Scraping helps bridge that gap. It allows us to introduce mechanical input in a way that is tolerable, which can then be followed by gradually increasing exercise-based loading without immediately flaring symptoms.
Think of it as creating a more favorable environment for the tendon to accept load again. Instead of jumping straight into strengthening and irritating the tissue further, we prepare the tendon so that strengthening actually becomes productive instead of painful.
Part 3: What to Expect During and After Scraping
During the Treatment
- You will feel mild discomfort at worst. A sensation of pressure and friction, not sharp pain.
- We target specific areas based on your presentation: the supraspinatus tendon directly, the deltoid fascia, the periscapular muscles (infraspinatus, teres minor, subscapularis), and the trapezius (particularly the upper trap, which can elevate the scapula and reduce subacromial space).
- The scraping is typically followed immediately by a few gentle loading movements (like external rotation with light resistance) while we maintain the compressive tension. This pairing allows the tendon to experience load while in a mechanically optimized state.
After the Treatment
- You may notice mild redness or bruising at the treated area. This is normal and expected.
- Some patients experience soreness that day or the following day, similar to the sensation after a good workout.
- This soreness typically resolves within 24-48 hours and is followed by a noticeable improvement in pain-free range of motion.
In many cases, patients also notice subtle changes immediately; less hesitation when lifting the arm, smoother motion, or reduced “catching” during overhead movement. These changes are not just placebo; they reflect a temporary reduction in sensitivity combined with improved tissue mobility.
Consistency matters here. One session can create a noticeable difference, but lasting change typically comes from a series of treatments paired with progressive rehab. The goal is not just short-term relief, it’s building long-term tolerance so the shoulder can handle real-life demands again.
Part 4: Who Should Wait (And When to See Us First)
Scraping is not for every stage of injury. Here’s our clinical guidance:
Hold off on scraping if:
- Your injury is less than two weeks old. We wait for the initial acute healing phase to begin before adding external mechanical load. This conservative approach allows the tendon’s intrinsic repair mechanisms to start on their own.
- You have a full-thickness tear (as discussed above).
- You have significant night pain that wakes you up from sleep, regardless of position. This is a red flag that may indicate a more serious condition (calcific tendinopathy, full-thickness tear, or inflammatory arthritis). Pain only when lying on the affected side is mechanical and not a red flag.
- You have significant weakness (e.g., unable to lift your arm against gravity) or traumatic onset after a specific injury.
- You have failed 6+ weeks of conservative care without improvement. This may warrant further imaging or a surgical consultation.
We are a good fit if:
- You have pain with overhead reaching, but full range of motion is present.
- Your pain has been present for more than two weeks but less than several months.
- You have no red flags (significant night pain, weakness, traumatic onset).
- You are motivated to do the necessary rehab to complement the manual therapy.
Another key factor we look at is irritability. If your shoulder pain spikes significantly with minimal movement or lingers for hours after activity, your tendon may not be ready for aggressive loading yet. In these cases, scraping can be especially helpful as a starting point because it allows us to introduce stimulus without overwhelming the tissue.
Part 5: The Evidence (Briefly)
The research on IASTM for rotator cuff tendinopathy is promising but still evolving. Studies have shown that IASTM can increase soft-tissue extensibility, improve joint range of motion, and reduce pain through sensory receptor activation. Clinical trials are actively investigating whether combining IASTM with conventional physiotherapy provides superior outcomes to exercise alone.
What we know now: Scraping is not a standalone magic bullet. It is most effective when integrated into a comprehensive plan that includes progressive loading exercises, movement retraining, and (when appropriate) return-to-sport or return-to-activity programming.
The best current evidence suggests that the addition of IASTM to a standard rehab protocol may accelerate pain relief and improve function, particularly in the early to middle stages of recovery when loading tolerance is low.
It’s also worth noting that tendon healing is not a straight line. Pain can fluctuate even when progress is being made. A well-structured plan accounts for this by adjusting load, intensity, and frequency over time rather than chasing pain-free movement immediately. Scraping fits into this model by helping manage symptoms while still allowing forward progress.
Part 6: Is This for Athletes or Everyone?
Both.
For athletes (throwers, swimmers, tennis players, overhead athletes): Dynamic overload is often the primary driver. Scraping can help calm the acute reactivity of the tendon while you continue to work on the underlying biomechanics: scapular control, thoracic mobility, and rotator cuff strength. This is the foundation of returning to sport.
For non-athletes (desk workers, older adults, weekend warriors): Chronic impingement from posture and movement dysfunction is often the primary driver. Scraping helps address the local tendon irritation while we work on the mechanical environment (thoracic extension, scapular retraction, and shoulder mobility).
In both cases, the goal is the same: reduce pain, improve function, and build capacity.
The difference is in how we progress you. Athletes may move toward higher-speed, higher-load activities like throwing or overhead lifting. Non-athletes may focus more on daily function: reaching overhead, carrying groceries, or sleeping without pain. The end goal isn’t just “less pain,” it’s getting you back to doing what actually matters in your life.
Ready to See if Scraping Is Right for Your Shoulder?
If you’re in Hopkins, Minnetonka, or St. Louis Park and you’ve been living with that pinch every time you reach overhead, we can help. We’ll perform a thorough assessment to confirm rotator cuff tendinopathy (not something else), rule out red flags, and determine if scraping is an appropriate first-line treatment for your presentation.
You don’t have to keep guessing what’s going on with your shoulder or cycling through treatments that only partially help. Getting clear on the diagnosis and having a structured plan can make a significant difference in how quickly and confidently you recover.
Schedule a visit at Redbird Wellness to discuss your shoulder pain and explore whether scraping (IASTM) is the missing link in your recovery.